The introduction of modern medical science that paralleled economic growth was connected to a national interest in health that subsequently led to an increase in life expectancy. Life expectancy in Korea, as a result of an abundance of well-trained medical personnel, hightech equipped medical facilities, and a systemically maintained health screening system, is shown to be very high compared to the rest of the world. Above all, the introduction of a universal health insurance system allows all citizens to enjoy health insurance benefits. However, there are problems, such as increased medical expenses due to an aging population and a health span (the number of years that one lives in good health) that is shorter than the increasing life expectancy—in other words, people are living longer, but they are spending a greater percentage of their lives not in good health, as are also seen in many other countries. In addition, there are also a rising number of health problems that need solutions, such as new types of diseases, differences between metropolitan and rural areas in health care access, and health problems associated with lifestyle changes.
Government expenditures on health and various types of welfare by age, gender, and economic status have steadily increased. But these increases in expenditures are a financial burden to the government; the slowdown in economic growth, the rapidly aging population, and the decline in birth rates have become urgent problems that need to be solved.
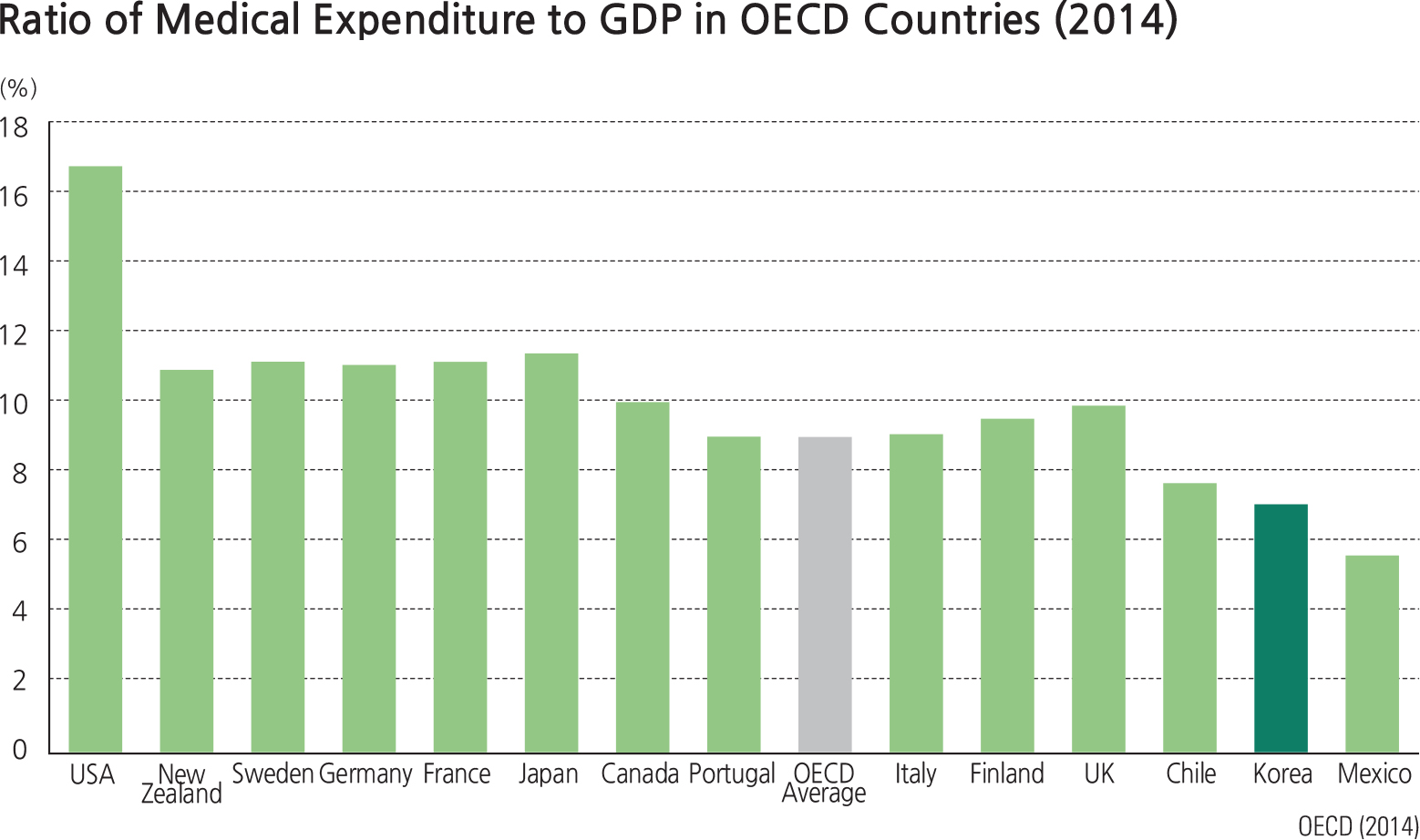
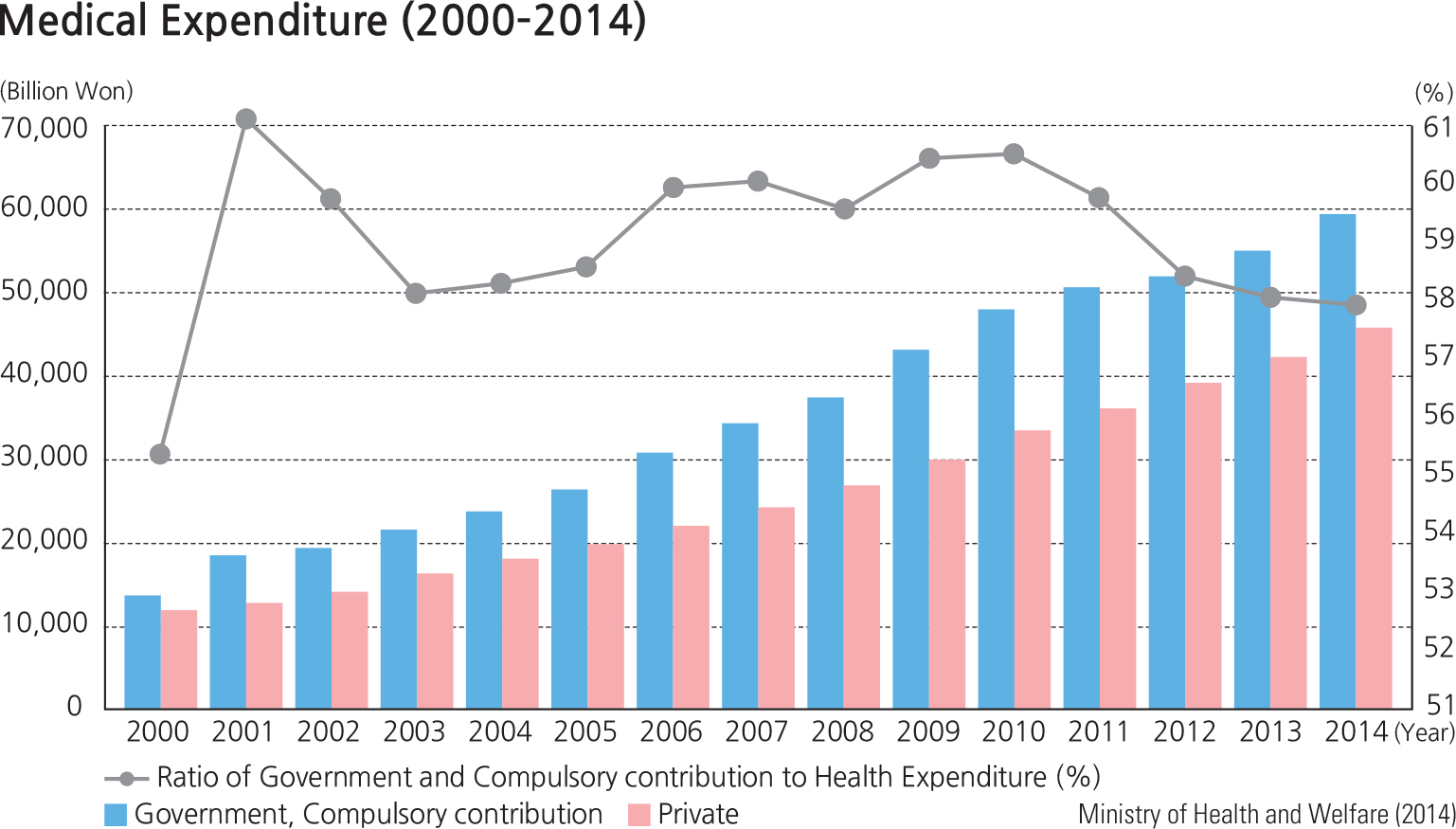
Medical expenditures as a percentage of Korean GDP are about 7 percent, lower than that of major countries of the OECD. However, medical expenditures have constantly increased as a result of an aging population and the increased interest in health care and a better understanding of new knowledge in health care. Medical expenditures are classified into two categories: 1) expenditures of government and compulsory contribution and 2) the private financial resources of private insurance and personal expenses. In the case of medical expenses, public financial resources had steadily increased for many years, but have begun to decline recently. An important issue for Korea is how to balance demands for increased health care spending with demands for fiscal sustainability by the government. Korea is very famous for well-trained medical personnel. The number of medical doctors and nurses is steadily increasing, and excellent medical personnel are being educated at all levels in colleges and universities, but the number of doctors and nurses per 1,000 people is relatively lower than that of other OECD countries.
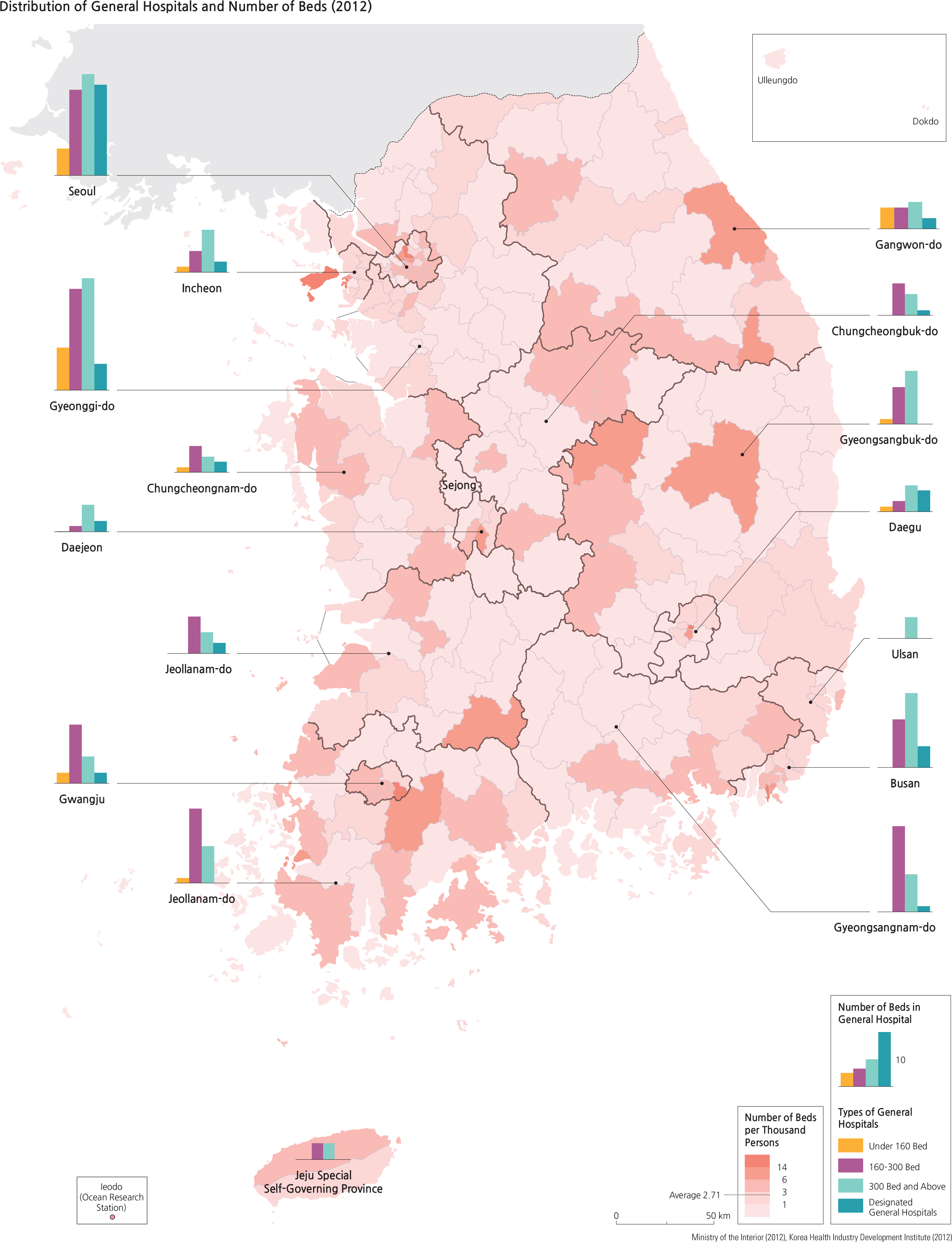
Medical institutions in South Korea are largely divided into clinics, small hospitals, and general hospitals, depending on the size of the institution. Mild diseases are treated at widely distributed clinics and small hospitals by specialized doctors. Serious illnesses or diseases are treated at the higher medical institutions, such as at a (major) general hospital. As many dental clinics are also widespread, access to dental clinics is good, too. Oriental medicine hospitals and clinics provide medical services based on oriental medicine. Medical access has greatly increased because general clinics and small hospitals are evenly distributed nationwide, while general hospitals are mainly distributed in metropolitan cities.
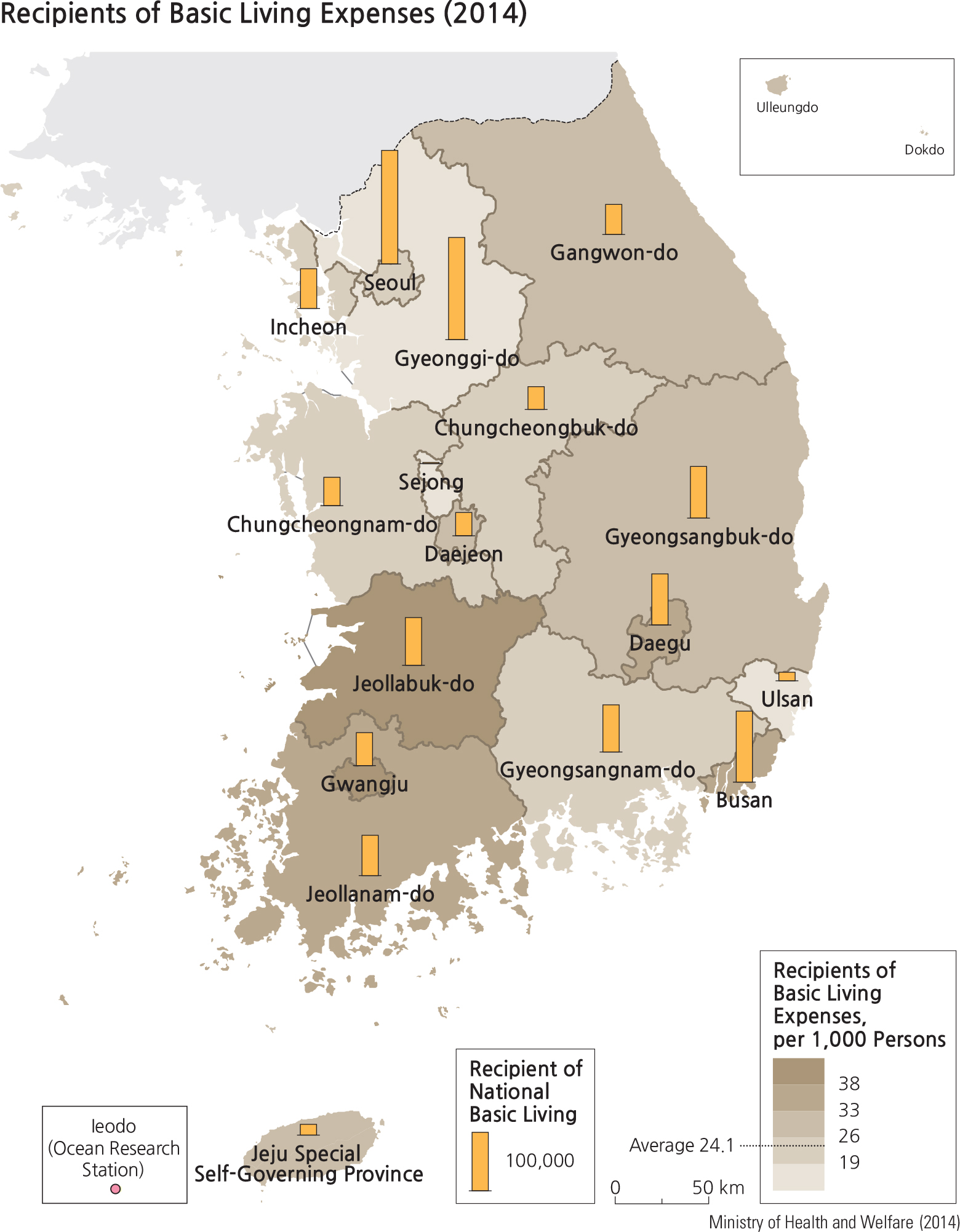
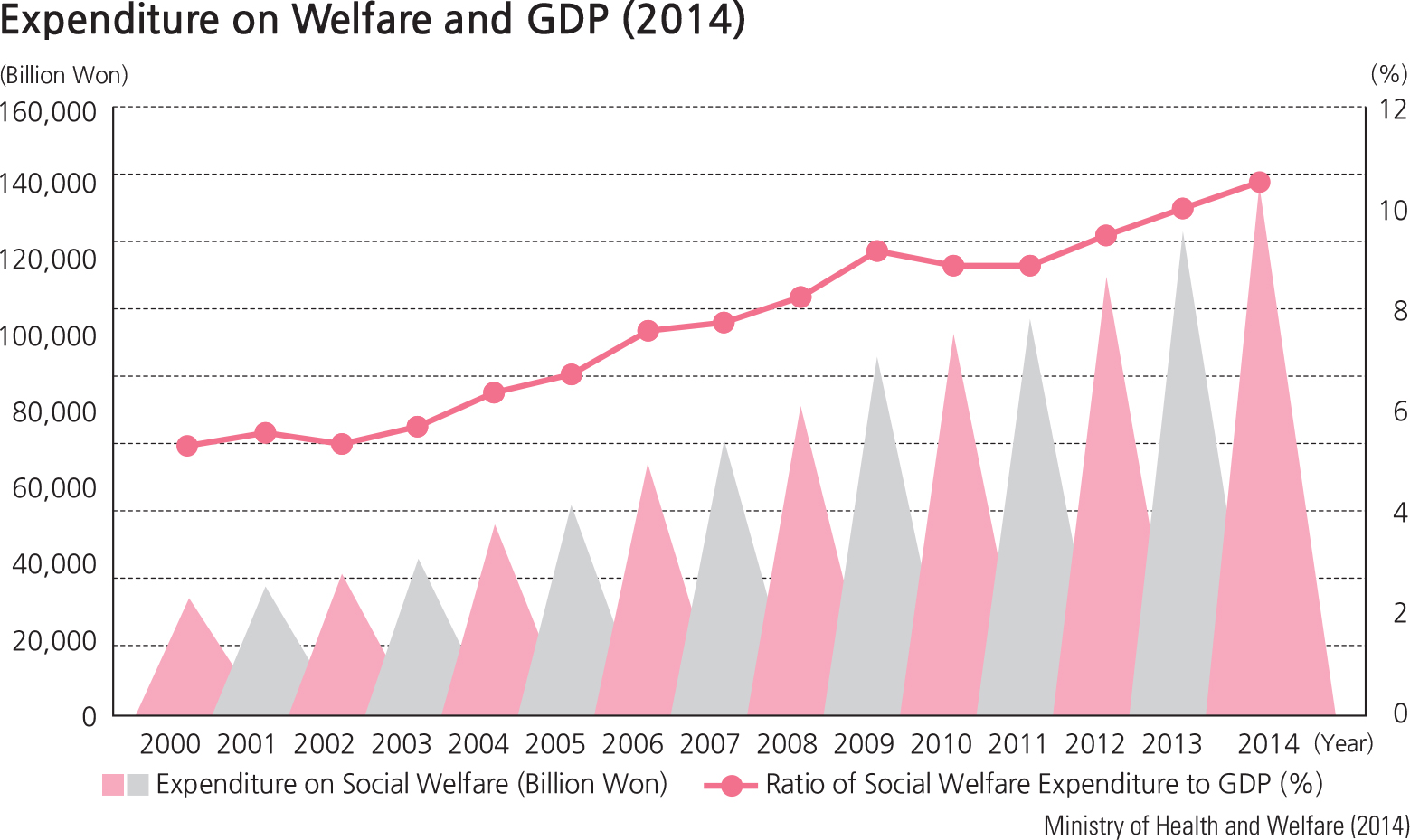
Social welfare related government expenditures are allocated according to welfare categories such as poverty, disabilities, women, children, and the elderly, or to sectors such as housing and labor. Recently, welfare in Korea hasemerged at the center of political debate. Various debatesrelate to such issues as the range of welfare services offered, the appropriate level of welfare, welfare-relatedgovernment expenditures in terms of fiscal soundness, and the priority of welfare spending. Whereas the growth of thenational economy has been a longstanding political issuethat requires national resources, recent political focus hasconcentrated on the expansion of social welfare and the maintenance of fiscal soundness. Recent welfare-related expenditures have consistently increased. The sum of social welfare expenditures in the statutory private and public sectors have substantially increased every year. The ratio of social welfare expenditure to GDP has exceeded 10 percent in recent years; but this ratio is still lower than that of other OECD countries (20 to 30 percent in some European states). Although this difference should be considered in the context of the proportion of elderly in the population and differences in social welfare policies, the likelihood that social welfare expenditure in Korea will continue to increase in the futureis strong. With the increase in social welfare spending, therelated budget is also steadily increasing.
The 2014 Recipients of Basic Living Expenses map is constructed from data based on provincial and metropolitanadministrative units. Therefore, the statistics are not finelydetailed. In other words, the spatial variations of which -si/-gun/-gu district receives more expenses are not identified insuch a generalized map.
Brief Interpretation of the Map
As the title indicates, the 2012 Distribution of General Hospitals and Number of Beds map shows two separate sets of statistics. While clinics that are designed to treat general or minor illnesses are abundantly available throughout the entire nation, general hospitals that treat more serious health problems are mostly located in or near urban centers. Because population in urban centers is high, the ratio of the number of beds to population is relatively low in urban areas while modestly higher in rural areas. This does not mean that there is necessarily an inadequate number of beds in urban areas.
Do you think that the Korean government should invest more funds in building general hospitals in rural areas or is it a higher priority to find ways to increase the overall health care budget? Even though the spatial distribution of general hospitals are mostly in urban areas, how accessible are they? Is distance a critical factor here for rural residents, particularly in emergency care and trauma situations?